It is her first child.
She has been at this for eleven hours. Nothing in her life has prepared her for this—not the books, not her mother’s careful stories, not the classes with the pillows on the floor. The pain is a living thing, and it has been winning.
She is exhausted and frightened and, at this agitated moment, furious at her husband, who is standing exactly where she told him to stand and doing exactly what she asked him to do and somehow that is not helping at all.
He doesn’t move. He stays. He holds her hand when she lets him.
—
The girl who would one day change how this progressed was born in Westfield, New Jersey, on June 7, 1909. The youngest of three children. Her name was Virginia.
Her father, Charles, was a business executive by day and something harder to categorize by night—an amateur astronomer, an inventor, a man with a basement laboratory full of radio equipment and possibility. He used that equipment during the First World War to expose an enemy espionage ring. From his basement in Westfield, he had recorded German coded transmissions from a wireless station on Long Island—messages guiding U-boats to Allied ships. The government seized the station. The sinking of Allied vessels slowed.¹
One man, a basement, a homemade device, wax cylinders.
Virginia’s father.
He was, in other words, a man who paid close attention to things, and who believed that careful observation could change outcomes.
Virginia learned this from him early.
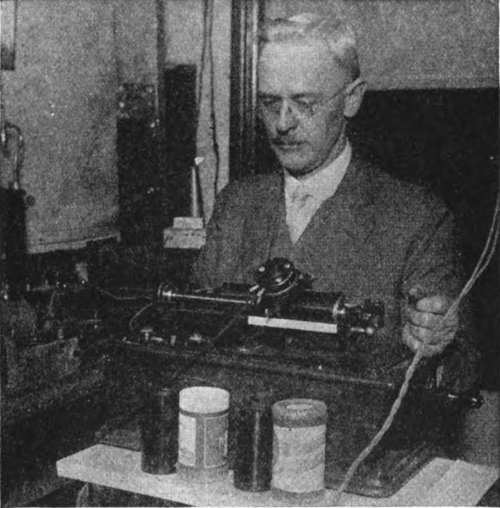
Charles A at radio
She learned music too. The violin first, then others. The family made music together the way some families play cards—naturally, regularly, as a matter of course. Virginia took to it with the same focus she took to everything. Precise, patient, serious about the craft.
But there was something else shaping her, something quieter and harder. She had two older brothers. Charles, the eldest, died before his fifth birthday—tuberculosis, 1904, five years before Virginia was born. The other brother, Lawrence, was chronically ill throughout childhood. Virginia grew up in a house that knew illness intimately. A house that understood, in the most personal way possible, that medicine was not academic. That it was urgent. That it mattered.
By the time she graduated from Westfield High School in 1925, she knew exactly what she wanted to do. She was going to be a doctor.
—
The room is loud, then louder. The pain crests into something beyond pain—something enormous and final and completely out of her control. She has never felt so alone inside her own body.
Then—
Now.
A boy.
The chaos of arrival fills the room—voices, hands, movement, light. The mother reaches. The father leans forward from wherever he has planted himself, at once both useless and essential.
And then, in the space where a cry should be—
Silence.
Not the silence of an empty room. The silence of a room full of people listening for one specific sound, and not hearing it.
The father looks at the nurse. The nurse does not look back. She is already moving—calm, purposeful, unhurried in a way that is itself a kind of urgency.
She reaches for the bulb syringe.
It is not a dramatic instrument. It fits in one hand. It does its small, essential work quietly—clearing the airway, mucus, making room for what needs to happen next.
A gentle tap on the sole of a very small foot.
Nothing.
A brush against a tiny cheek.
Nothing.
The father has stopped breathing. The mother’s hand finds the rail and grips it.
Where is the cry?
—
She got there the hard way.
With the help of scholarships and whatever work she could find—waitressing, library shifts, anything—Virginia enrolled at Mount Holyoke College in South Hadley, Massachusetts, one of the great women’s colleges of the Northeast. She was known there as “Jimmy.” The girl who did it all. She played violin and cello in the college orchestra, ran herself ragged with activities, and wrote home to her parents with characteristic understatement: I’m very well and happy but I haven’t one minute even to breathe.
She graduated in 1929 with a degree in zoology, minors in physiology and chemistry, and a destination already fixed in her mind. Columbia University College of Physicians and Surgeons. New York City.
She arrived just as the Depression arrived.
The money ran out almost immediately. She borrowed to stay in school, accumulating debt with the same quiet determination she applied to everything else. Around her, the country was coming apart. In New York City, even male surgeons were struggling to find work.
None of it stopped her.
In 1933, Virginia graduated fourth in her class of ninety. One of only ten women among them. She had earned her place at the table by every measure that existed. Now she intended to be a surgeon.
Three months earlier, Franklin Roosevelt had told a frightened nation the only thing it had to fear was fear itself. Virginia could have told him that.
—
Seconds are passing.
The father knows this because he is counting them—a habit, something to give a mind with nothing useful to do. He is watching the nurse with an intensity that has nowhere else to go. She is still moving—quietly, methodically—and her face is giving him nothing.
This is, he will later understand, a skill. The carefully neutral expression. The unhurried hands. The voice, when it comes, measured and calm. These are things you learn, things you practice, things you bring into a room like this because the parents are reading every signal you send and you cannot afford to send the wrong one.
The mother is spent. Wrung out. She has nothing left and she knows it and she reaches anyway, toward the small still form across the room, because—what else is there to do.
More seconds.
The nurse does not look up.
The father thinks: should I say something? He thinks: is this normal? He thinks: someone tell me this is normal.
Nobody tells him anything. They are all too busy doing what needs to be done—what they were trained to do, what they have done before, what they will do again. Their calm is not indifference. It is something much more valuable than that.
It is competence. It is preparation. It is, though no one in this room knows it, the gift of a woman named Virginia.
—
She wanted to be a surgeon. She had earned it. By every clinical measure, every academic standard, she belonged in an operating room.
Allen Whipple, the chairman of surgery at Columbia, thought otherwise. He had watched women attempt surgical careers and seen them fail—not for lack of skill, but for lack of opportunity, for lack of welcome, for lack of a world willing to make room for them. And then—they were lost to medicine. Brains and talent leaving medicine.He was not cruel. He was, in his way, practical. He steered her elsewhere.
He suggested anesthesiology.
It was not a compliment. Anesthesia in the 1930s was barely a specialty at all—underpaid, underrespected, largely performed by nurses. Surgeons considered anesthesiologists mere support staff. The suggestion was, in the language of the time, a consolation.
Virginia took it anyway.
She trained under Ralph Waters at the University of Wisconsin—the first formal anesthesiology department in the country. Then under Emery Rovenstine at Bellevue Hospital in New York. She was rigorous and gifted and utterly serious about a field that almost nobody else was taking seriously yet.
In 1938 she returned to Columbia as director of the newly formed division of anesthesia. She was, for years, its only member. Surgeons dismissed her. Recruitment was nearly impossible. The pay was low, the prestige lower.
She built it anyway.
By 1949 the division had become a department—a real one, with residents, with research, with standing. Something of consequence. Virginia had built it from nothing, with her own hands, her own energy, her own devotion, over eleven years.
They did not give her the chairmanship. Too little research, they said.
They gave her a full professorship instead—the first woman ever to hold that rank at Columbia’s College of Physicians and Surgeons.
She accepted it. She kept working.
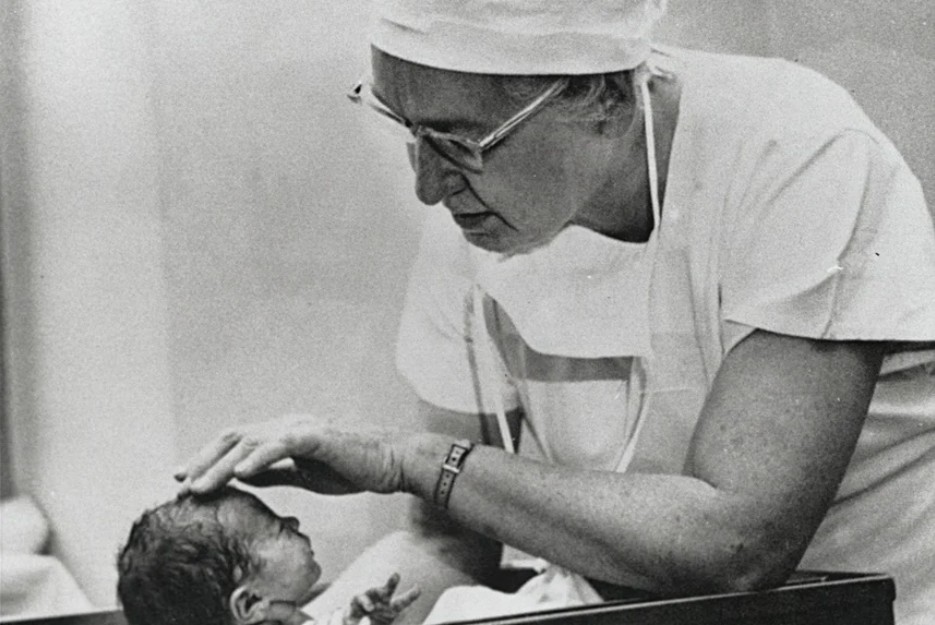
Virginia with new born
Her hands, all this time, were precise. Musician’s hands. She had always been good with them—the violin, the viola, the instruments she eventually learned to build herself. A patient had taught her once, and she had gone home and built a cello. Then a violin. Then a viola. Because if something was worth doing, it was worth understanding completely, from the inside out.
Those same hands were now in delivery rooms. More and more, she found herself drawn there—to the wondrous drama of birth, to the moment of arrival, to the newborn who entered the world and either announced itself or did not. She was watching something that nobody was measuring carefully enough.
The newborn, in 1949, was almost an afterthought. If the baby cried, it was fine. If it didn’t, someone worried. There was no standard. No protocol. No systematic way to look at a new human being and say:
This one needs help, and here is why, and here is what we do.
Virginia thought that was unacceptable.
—
The nurse reaches for the bulb syringe again.
Another gentle tap on the sole of a very small foot.
A gasp.
Small. Wet. Indignant.
Then the cry.
The father lets out a sound—something between a laugh and a sob, preceded by a single helpless syllable. Whew. Then his shoulders come down from wherever they have been for the last eleven hours, and he is laughing and crying at the same time, which he has never done before in his life.
The mother closes her eyes. Opens them. Reaches.
“Is it over?”
It is over.
One minute passes. The nurse looks up and calls across the room.
“Apgar—eight.”
The parents look at each other. Eight what? Out of what? The nurse is calm. The doctor is calm. Eight must be good.
The baby is placed on the mother’s chest.
This is the moment. This is the one she couldn’t imagine, no matter how many times she tried. This small warm furious person, here, outside, real. She puts both hands around him and doesn’t say anything at all. Tears form and roll.
The father leans in. His face is a ruin—in the best possible way.
Four more minutes pass. Nobody is counting except the nurse.
“Apgar—nine.”
And that’s when the room fills up. The attendants’ eyes smile first—smiles behind their masks, crinkles at the corners. Shoulders that have held tension too long go soft. The vibe is contagious. Laughter comes, and tears, and the overwhelming joy that has no name and needs none. The father is useless again, gloriously, indefinitely useless, laughing and crying and not caring at all.
He wipes his face. He looks at the nurse.
“Apgar—what’s that?”
The nurse looks up. She has answered this question so many times before.
“It’s an aggregate score. Five categories, zero to two points for each.
A is for Appearance.
P is for Pulse.
G is for Grimace.
A is for Activity.
R is for Respiration.”
The father nods. Looks at his son. Looks back.
“What’s it called?”
The Apgar score.²
And now, meet Virginia Apgar.
—
The story, as it is told, begins at breakfast.³
It is 1949. A medical student, eating with Virginia Apgar at the Columbia faculty dining room, asks an offhand question. How would you even begin to systematically evaluate a newborn? Virginia picks up a napkin. Writes down five criteria. Assigns each a value of zero, one, or two.
That was it. That was the whole thing.
 She presented it formally in 1952. Published it in 1953. The medical establishment received it with the characteristic resistance that greets anything that makes people wonder why they hadn’t thought of it themselves. Then, slowly, hospitals began to adopt it. Then more hospitals. Then all of them.
She presented it formally in 1952. Published it in 1953. The medical establishment received it with the characteristic resistance that greets anything that makes people wonder why they hadn’t thought of it themselves. Then, slowly, hospitals began to adopt it. Then more hospitals. Then all of them.
By the late 1950s Virginia had personally attended more than 17,000 births. She had seen what the score could do—not just identify distress, but prompt immediate, systematic response. Babies who would have slipped away in the old world of vague impressions and missed signals were, in this new world, caught. Measured. Treated. Sent home
The March of Dimes had conquered polio. The Salk vaccine had seen to that. But Virginia Apgar had been in delivery rooms for twenty years. She had seen what the score caught—and she had seen what it couldn’t fix. The babies who arrived broken in ways no number could address. The ones whose parents would spend a lifetime loving them through difficulties nobody planned for.
Those children needed someone in their corner too.
She redirected the organization entirely—away from polio, toward birth defects and premature birth. She became its most visible champion, traveling constantly, speaking everywhere, raising money with the energy of someone who understood exactly what the money was for.
She understood it completely.
She never slowed down. There was always more to do, always another audience that hadn’t heard the message yet, always another baby who needed someone paying attention.
Virginia Apgar died on August 7, 1974, at Columbia-Presbyterian Medical Center. She was 65 years old. She had been working until her very end.
She was buried in Westfield, New Jersey. Where she started.
—
She never married.
She had no children of her own.
And yet—every child born in a modern hospital, in every country where medicine has reached, entered this world under her watchful, numbered care. The nurse who called those numbers across the delivery room tonight was following a protocol Virginia Apgar wrote on a napkin many decades ago.
Seven. Eight. Nine. Ten.
Millions of children. Tens of millions. Hundreds of millions, across seven decades, with no end in sight.
All of them, in some sense, hers.
Joe Girard © 2026
Thank you for reading. As always, you can add yourself to the notification list for newly published material by clicking here . Or emailing joe@girardmeister.com
¹ Charles Emory Apgar, Virginia’s father, recorded coded German transmissions from the Sayville Wireless Station on Long Island in 1915, providing evidence that led the U.S. government to seize the facility. Sources: “Charles E. Apgar, Helped Trap Spies: Intercepted Radio Signals Guiding U-Boats in 1915,” New York Herald Tribune, August 19, 1950; “Charles E. Apgar, Radio Expert, 86,” New York Times, August 19, 1950, p. 12. The Henry Ford Museum holds the original homemade recording device. See also: Charles Apgar, apgarfamily.org/node/28.
² The APGAR backronym—Appearance, Pulse, Grimace, Activity, Respiration—was not Virginia’s own invention. The criteria were chosen on medical merit; the fact that their initials spelled her name was either cosmic coincidence or a quiet tribute from colleagues, depending on who is telling the story. Virginia herself never claimed it. Her name was simply there, hiding inside the thing she built, waiting to be noticed.
³ The breakfast conversation is widely cited but may be apocryphal. It has the quality of legend—a great idea arriving casually, on ordinary materials, between bites of eggs. Whether it happened exactly this way or not, something like it happened. The napkin, real or imagined, changed everything.
A few of many sources
Charles Apgar, Apgar Family Association: apgarfamily.org/node/28
Virginia Apgar, Saturday Evening Post, February 11, 2025: saturdayeveningpost.com
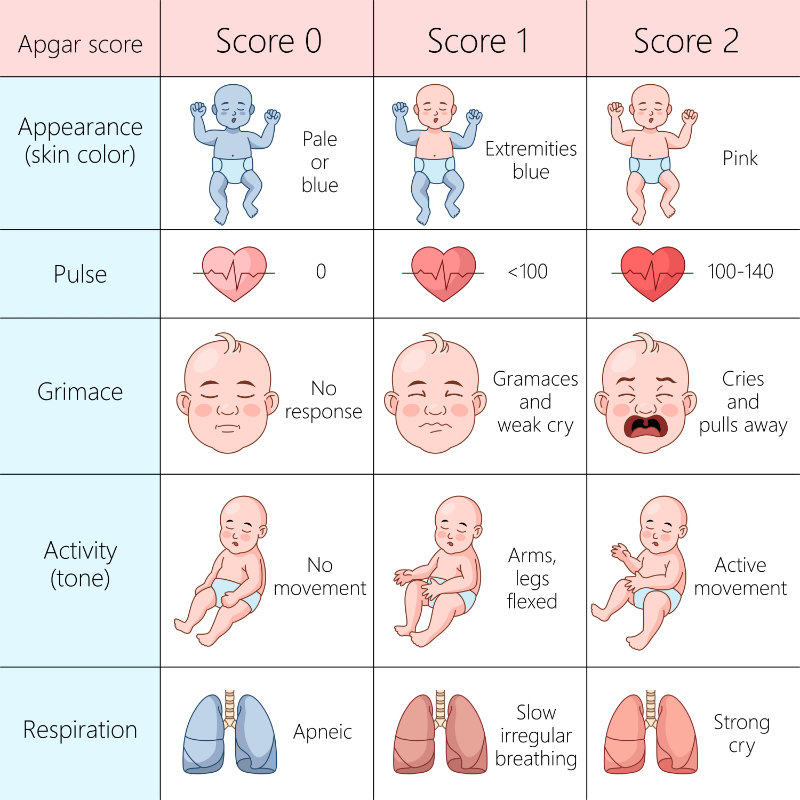
Apgar score chart evaluating the health of newborns, appearance, pulse, grimace, activity, and respiration diagram hand drawn schematic raster illustration. Medical science educational illustration